


















Step 1 of 4
Définition
La grande variabilité de réponse aux antiplaquettaires et l’intense blocage requis après SCA ou PCI, particulièrement dans les cas de stents à haut risque, rendent nécessaire de pouvoir quantifier la réponse des patients à ces médicaments. Il existe bien des tests génétiques pour le principal allèle inactif des cytochromes hépatiques responsables du métabolisme du clopidogrel (CYP2C19*2), mais ce phénomène n’explique que 12-20% de la variabilité dans la réponse à la substance [13]. Il paraît donc souhaitable de pouvoir évaluer l’agrégabilité plaquettaire d’un malade afin de sélectionner le traitement optimal en fonction de sa réponse aux inhibiteurs, que ce soit le choix du mode de revascularisation ou celui de l’antiplaquettaire et de son dosage. Ceci appelle trois remarques [5,6,7].
- L’agrégabilité plaquettaire est un phénomène complexe et multifactoriel, dont il est malaisé de tester le degré d’inhibition avec un seul examen standard, rapide et univoque.
- Plusieurs examens sont disponibles, mais ils évaluent des mécanismes différents du fonctionnement des plaquettes ; leur degré de cohérence est modeste.
- Il n’existe qu’un consensus récent et que des recommandations provisoires (classe IIa, degré d’évidence B) sur l’impact clinique de ces examens et sur leurs valeurs-seuil au-delà desquelles le risque de complication devient très élevé [1,3,12].
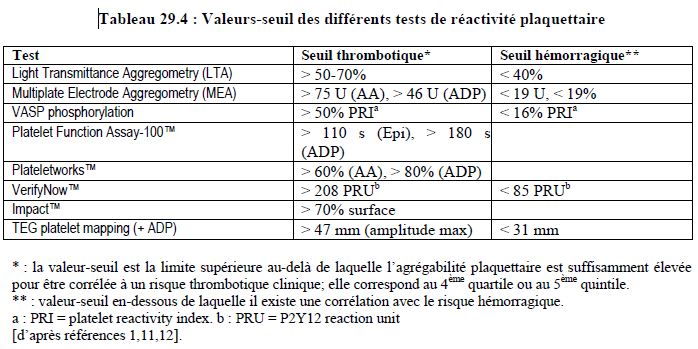
Les principaux tests utilisés en clinique sont résumés dans le Tableau 29.3 et leur point d’impact illustré dans la Figure 29.11 ; les valeurs-seuil associées aux complications cardiovasculaires sont mentionnées dans le Tableau 29.4 [2,4,8,9,10,12].
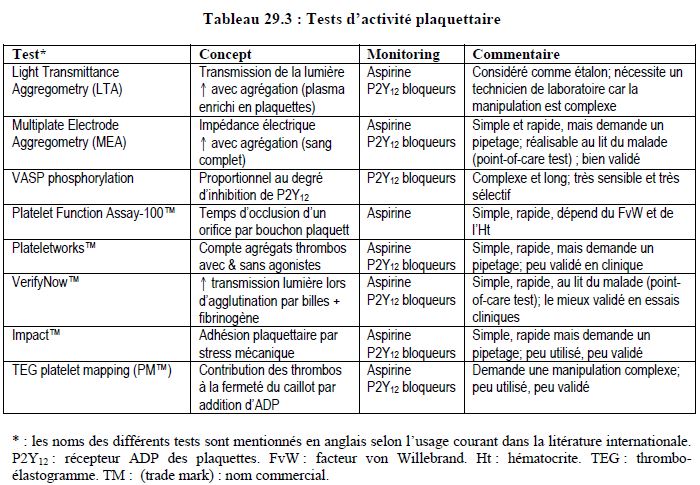
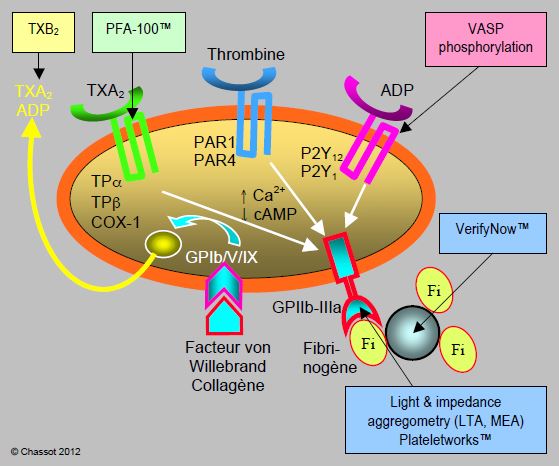
Figure 29.11 : Points d’impact de différents tests d’agrégation plaquettaire. Les examens dont le point d’impact est le récepteur GP-IIb/IIIa (LTA, MEA, VerifyNow™, Plateletworks™) ne sont valables qu’en l’absence d’inhibiteurs propres de ce récepteur (abciximab, tirofiban, eptifibatide).
© CHASSOT PG, DELABAYS A, SPAHN D Mars 2010, dernière mise à jour Août 2018
Références
- ARADI D, STOREY RF, KOMOCSI A, et al. Expert position paper on the role of platelet function testing in patients undergoing percutaneous coronary intervention. Eur Heart J 2014; 35:209-15
- FAVALORO EJ, LIPPI G, FRANCHINI M. Contemporary platelet function testing. Clin Chem Lab Med 2010; 48:579-98
- FERRARIS VA, SAHA SP, OESTREICH JH, et al. 2012 update to the Society of Thoracic Surgeons Guidelines on use of antiplatelet drugs in patients having cardiac and noncardiac operations. Ann Thorac Surg 2012 ; 94 :1761-81
- FERREIRO JL, SIBBING D, ANGIOLILLO DJ. Platelet function testing and risk of bleeding complications. Thromb Haemost 2010; 103:1128-35
- FINTEL DJ. Oral antiplatelet therapy for atherothrombotic disease: overview of current and emerging treatment options. Vasc Health Risk Manag 2012; 8:77-89
- GEISLER T, GAWAZ M, STEINHUBL SR, et al. Current strategies in antiplatelet therapy - Does identification of risk and adjustment of therapy contribute to more effective, personalized medicine in cardiovascular disease ? Pharmacol Ther 2010; 127:95-107
- GOROG DA, FUSTER V. Platelet function tests in clinical cardiology. Unfulfilled expectations. J Am Coll Cardiol 2013; 61:2115-29
- KULICZKOWSKI W, WITKOWSKI A, POLANSKI L, et al. Interindividual variability in the response to oral antiplatelet drugs: a position paper of the Working Group on antiplatelet drugs resistance appointed by the Section of Cardiovascular Interventions of the Polish Cardiac Society, endorsed by the Working Group on Thrombosis of the European Society of Cardiology. Eur Heart J 2009; 30:426-35
- MICHELSON AD. Methods for the measurement of platelet function. Am J Cardiol 2009; 103S:20A-26A
- PRICE MJ. Bedside evaluation of thienopyridine antiplatelet therapy. Circulation 2009; 119:2625-32
- SILLER-MATULA JM, TRENK D, SCHRÖR K, et al. How to improve the concept of individualised antiplatelet therapy with P2Y12 receptor inhibitors – is an algorithm the answer ? Thromb Haemost 2015; 113:37-52
- TANTRY US, BONELLO L, ARADI D, et al. Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding. J Am Coll Cardiol 2013 ; 62 :2261-73
- WANG L, McLEOD HL, WEINSHILBOUM RM. Genomics and drug response. N Engl J Med 2011; 364:1144-53
29 Les antiplaquettaires en chirurgie cardiaque et non-cardiaque
- 29.1 Physiopathologie des thrombocytes
- 29.2 Antiplaquettaires classiques
- 29.3 Nouveaux antiplaquettaires
- 29.4 Tests d'activité plaquettaire
- 29.5 Antiplaquettaires en périopératoire
- 29.5.1 Situation
- 29.5.2 Antiplaquettaires et maladies cardiovasculaires
- 29.5.3 Arrêt des antiplaquettaires
- 29.5.4 Risque hémorragique peropératoire
- 29.5.5 Balance des risques
- 29.5.6 Recommandations pour la chirurgie non-cardiaque
- 29.5.7 Recommandations pour la chirurgie cardiaque
- 29.5.8 Antiplaquettaires et anesthésie loco-régionale (ALR)
- 29.5.9 Transfusion plaquettaire et intervention pharmacologique
- 29.6 Conclusions